As you can imagine, we are sent a huge number of radiographs of stifles to evaluate. Some good, some not so good!
Radiographs are the most valuable and straightforward imaging tool to evaluate the stifle. To diagnose likely cruciate disease radiographically, we are looking for evidence of effusion and osteoarthritis in the form of peri-articular new bone. We may also be able to see evidence of medial fibrosis “medial buttress”. It is also important to rule out other less common causes of stifle problems, like a bone tumour.
In order to get the most information from stifle radiographs, it’s important that the views are well positioned.
The medio-lateral view should be positioned so that the femoral condyles are superimposed, and the body wall is clear of the whole of the stifle joint. This can be difficult in obese dogs and sometimes the creative use of a rope tie may be required. If the stifle is not straight on the medio-lateral view, it can be impossible for us to look for an effusion.
Figure 2. Rotated medio-lateral view, difficult to interpret
Our preferred position for a medio-lateral view is shown in the following pictures, and we recommend you try out this way of positioning if you are having difficulty getting straight medio-lateral views. Sometimes the position requires minor adjustment with a small foam pad under either the hock or the hip.
Figure 3A. Medio-lateral positioning
Figure 3B. Medio-lateral positioning
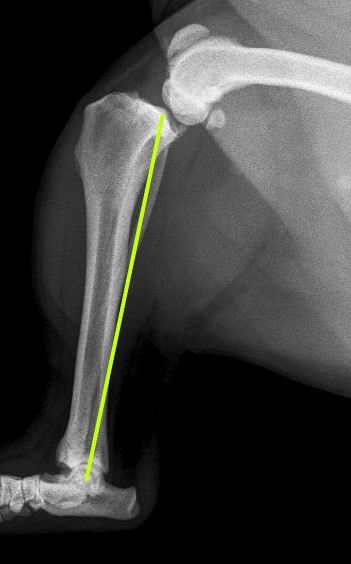
We also use the medio-lateral view to measure the “tibial plateau angle” which is important in planning a TPLO. In order to measure this angle we need the hock to be included in the radiograph, as the tibial long axis is defined as a line from the centre of the talus to the intercondylar eminence on the tibial plateau. The radiograph should be centred on the stifle, and the beam collimated out to include the hock.
Figure 4A. Tibial Axis
Figure 4B. Tibial plateau angle
The caudo-cranial view is best obtained in sternal recumbency. In this position, you can use the position of the paw, and palpation of the patella/tibial tuberosity to achieve a straight view. A good caudo-cranial will have the patella centrally overlying the femur and the fabellae bisected by the femoral cortices. You may need to keep the tail out of the way with a sandbag or tie.
Figure 5A. Caudo-cranial positioning
Figure 5B. Caudo-cranial positioning
Figure 5C. Rotated caudo-cranial view
Figure 5D. Straight caudo-cranial view view
Good quality radiographs help us to make a confident diagnosis and avoid the need for repeating radiographs on the day of surgery, keeping the anaesthetic as short as possible.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. This category only includes cookies that ensures basic functionalities and security features of the website. These cookies do not store any personal information.
Any cookies that may not be particularly necessary for the website to function and is used specifically to collect user personal data via analytics, ads, other embedded contents are termed as non-necessary cookies. It is mandatory to procure user consent prior to running these cookies on your website.